
Data sharing between different levels of the health system
Why health systems collect data
National governments maintain health information systems to inform and monitor the running of their health systems. The World Health Organization categorizes health information as one of six health-system building blocks alongside: service delivery; health workforce; access to essential medicines; financing; and leadership/governance.
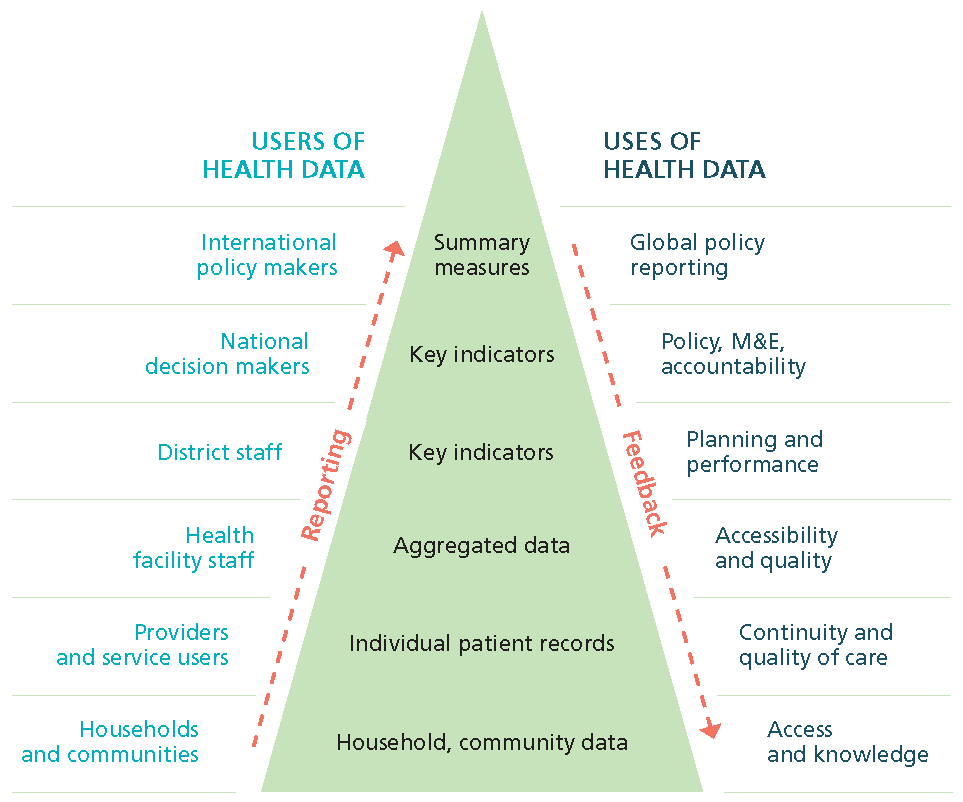
Health information systems operate at all administrative levels of the health system as the above figure demonstrates. Health informations systems collect and manage data:
- Inform individuals, communities, civil society groups, research organizations and the media about: population health status; and the availability of, access to and use of services by population sub-groups.
- Provide management record systems for managers at health facilities to: plan and assess service provision; guide procurement and staffing; claim and allocate financial resources; and maintain facility infrastructure, equipment and supplies, including medicines and diagnostics.
- Assist planners and managers at sub-national levels of the health systems (eg district) to: compile records-based data on notifiable conditions seen at health facilities for surveillance and effective response; track service coverage; coordinate service provision; allocate resources ;and implement, supervise and evaluate programmes across facilities and the populations they serve.
- Support managers and policymakers working at the national level to: set policy; develop programmes and monitor and evaluate health sector performance; and report indicators for country targets to international agencies.
In addition to working with national averages, policymakers need disaggregated data to highlight challenges facing particular population groups. For example: the poorest households; remote and marginalised groups; minorities; and vulnerable populations such as the elderly, persons living with a disability and ethnic minorities.
While countries need data primarily for national and local decision-making, they also report indicators to the World Health Organization and other international and regional organisations so that these agencies can monitor global progress towards Sustainable Development Goal targets, for example, and prepare global and regional policy and response.
National health information systems
The purpose of a national health information system is to coordinate:
- The collection, management, analysis and synthesis of data; and
- Dissemination of timely, quality and relevant information to decision-makers within the health system and beyond; and
- To account to the general public, tax payers and development partners.
System managers and analysts deliberately generate and analyse data to provide indicators about the health status of populations and functioning of the health system. They also provide evidence of determinants of health conditions and effective interventions.
The health information system mirrors the objectives and organizational structure of the health system. The health information system:
- Collects data from the health sector and other relevant sectors;
- Manages the data and ensures their overall quality, relevance and timeliness; and
- Converts data into information for health-related decision-making and advocacy.
Many non-governmental entities contribute data to run the health system. These include private and non-governmental health organisations, consumer watchdog groups and academic and research institutions.
When routine data are insufficient or unreliable, donor agencies have funded programme-specific data collection. For example: the Global Fund to fight AIDS, Tuberculosis and Malaria (GFATM), the United States (US) President’s Emergency Plan for AIDS Relief (PEPFAR), GAVI the Vaccine Alliance, and the Roll Back Malaria (RBM) partnership have developed disease specific information initiatives.
Statistical systems
The health sector is both a consumer of and contributor to information relative to other social and economic sectors.
A well-functioning health information system depends on activities undertaken within the health sector but in other sectors with responsibilities for statistical development. Thus, the health information system works within a multi-sectoral statistical system. Such interlinked systems cut across sectoral boundaries using data generated by the health system and data produced by other agencies.
National statistical systems
A national statistical system comprises the statistical organizations and units within a country that jointly collect, process and disseminate official statistics on behalf of national government. Some statistical systems are centralized in which the national statistical office coordinates publication of official statistics across sectors. Others are decentralized with each sector responsible for publishing it official statistics. Whether decentralized or centralized, the national statistical office coordinates governmental statistical activities.
Sectors contributing health data
Key contributors of health-related data are:
The national statistical office; census bureau; civil registration authority; and sectors generating, for example, data on: environmental pollution, occupational and road safety, food safety, production and standards, poverty, income distributions and economic growth.
Problems can arise when different sectoral agencies have overlapping mandates and responsibilities for data collection, management, analysis and reporting. For example, the health sector may collect data on births and deaths occurring in health facilities independently from the activities of the national civil registration system. Resulting differences in key indicators can undermine the credibility and trustworthiness of the data. The national statistical office can minimise these problems by coordinating statistical activities, determining standards and sharing technical expertise across the system.
Principles of Official Statistics
The United Nations Statistical Commission, representing chief statisticians from all member states, sets the standards which the national statistical office and other line ministries, including the ministry of health, must follow in producing official statistics. In particular, the Commission has laid out the ten Fundamental Principles of Official Statistics:
- Official statistics provide an indispensable element in the information system of a democratic society, serving the Government, the economy and the public with data about the economic, demographic, social and environmental situation. To this end, official statistics that meet the test of practical utility are to be compiled and made available on an impartial basis by official statistical agencies to honour citizens’ entitlement to public information.
- To retain trust in official statistics, the statistical agencies need to decide according to strictly professional considerations, including scientific principles and professional ethics, on the methods and procedures for the collection, processing, storage and presentation of statistical data.
- To facilitate a correct interpretation of the data, the statistical agencies are to present information according to scientific standards on the sources, methods and procedures of the statistics.
- The statistical agencies are entitled to comment on erroneous interpretation and misuse of statistics.
- Data for statistical purposes may be drawn from all types of sources, be they statistical surveys or administrative records. Statistical agencies are to choose the source with regard to quality, timeliness, costs and the burden on respondents.
- Individual data collected by statistical agencies for statistical compilation, whether they refer to natural or legal persons, are to be strictly confidential and used exclusively for statistical purposes.
- The laws, regulations and measures under which the statistical systems operate are to be made public.
- Coordination among statistical agencies within countries is essential to achieve consistency and efficiency in the statistical system.
- The use by statistical agencies in each country of international concepts, classifications and methods promotes the consistency and efficiency of statistical systems at all official levels.
- Bilateral and multilateral cooperation in statistics contributes to the improvement of systems of official statistics in all countries.
Data sources
The health information system brings together data from multiple sources at all levels of the health system, and from outside the health sector. Our description is consistent with the Measurement and Accountability for Health Roadmap.
Data about populations through:
- National decennial censuses that count the entire population and describe its demographic structure by geographic area and administrative level.
- Civil registration and vital statistics systems that continually record vital events such as births and deaths nationally or for specific administrative areas.
- National and local household surveys that describe, for example: health status, service coverage, health-related behaviours and risk factors, out-of-pocket spending on health, including equity dimensions of health status and service coverage, and population knowledge such as use of antibiotics and awareness of antimicrobial resistance.
Data from facility and community records
A health management information system provides the overall system for collecting these types of data:
- Medical records about patients and families seen at the health facility or in the community including disease registers.
- Registers of services provided by health facilities and programmes.
- Community-based systems such as community health worker registers.
- Health facility assessments designed to track: the availability and geographic distribution of public and private health facilities; the quality of infrastructure; availability of equipment and commodities; and readiness to offer specific services.
Public health surveillance systems operate locally and nationally, and draw on multiple sources of data to watch out for and respond to unwanted public health events that occur in the population.
Data from specialised systems
For example:
- Human resources for health information systems that enable countries to track, manage, and plan the health workforce so that the required health workers are available in the right place at the right time and that they are properly trained, remunerated and supervised.
- Systems of national health accounts which assist health system planning by describing the way in which money flows through the system, recording all income and expenditure.
- Drug and medical provisions systems to manage demand and supply, ensure drug safety and facilitate efficient procurement.
Other sources
Beyond the publicly managed health information system, other bodies contribute data to watch over the integrity of data and information available to policymakers.
- Private and non-governmental health organisations maintain information systems but are encouraged to link these with the public systems. Coverage of notifications of highly infectious and epidemic prone diseases from private sector providers is critical for surveillance and effective response.
- Consumer watchdog groups collect data to assess the quality of and complaints about the health services available to them.
- Data analysts trawl the web for health-related data to describe and predict trends in health status and healthcare.
- Academic and research institutions undertake assignments for governments and publish independent medical and public health research, supported by public and private funds.
Sharing the data
Not every country necessarily describes the sum of its information gathering as a health information system. But all countries collect and coordinate health and health-related data to develop and assess governments services and use some combination of the data sources we have described.
Preferably the government should make the data openly available to the general public and researchers once they have ensured privacy and confidentiality of individual records.
For example, the Finnish health information system aims to provide all users with free access to the data it collects. The system offers web-based portals with indicators and data for all three levels of its health system, which the government collects mainly through coordinated administrative registers and multiple surveys.
Governance and coordination
In 2015, the World Health Organization made recommendations on the importance of governance, emphasizing four features namely:
- Legal, institutional and policy frameworks, including harmonisation and coordination among entities involved in health information.
- Data standards, comprising core indicators with associated metadata and international classifications.
- Information system architecture, including semantic and technical or syntactic standards that enable different information sub-systems to work together in an interoperable way.
- Human resources and capacities for data collection, supervision and quality assurance, data curation, analysis, interpretation, and dissemination.
Country experiences in implementing data quality assurance frameworks indicate that it is essential to bring together interdisciplinary teams to design and manage an information system; these include subject matter staff, methodologists, and operations and systems experts. This is emphasised, for example, by Statistics Canada.
System assessment
To understand the reliability of country data, development partners and technical experts have developed health information system assessment tools. Some, such as the Health Metrics Network assessment tool, involve multiple stakeholders, and are too complex for monitoring purposes. Other tools are simpler but are primarily applied by external parties, limiting country involvement and ownership.
MEASURE Evaluation provides a health information system strengthening resources centre which includes a database of tools for assessing health information systems.
Challenges
The 2017 World Health Statistics report examined the 42 Sustainable Development Goal health-related indicators (counting UHC as one indicator) and judged CRVS to be the preferred (or equally preferred) source for 16 of them, population surveys for 22 and facility-based records for only six of the indicators. Many indicators also depend on population numbers enumerated by a decennial census. The report acknowledged that ‘very few’ of the 42 indicators ‘are adequately measured in most countries’.
We summarise some of the challenges:
- Low registration of births and deaths. Only one percent of the population of Asia and Africa currently lives in countries which have complete death registration
- Too many poorly coordinated surveys. Countries undertake disease and programme specific national surveys to meet donor reporting requirements, thus adding pressure on limited expertise and resources.
- Inadequately resourced under-performing facility-based and other record systems. For example, problems in: maintaining data quality and completeness; timeliness in reporting; and in stimulating usage of the information the facilities produce.
- Inconsistencies between values of indicators. Routine HMIS systems are beset by problems of bias and missing values – contributing to both the numerators and denominators of health indicators. While household surveys usually generate indicators of superior accuracy and reliability, this depends on the quality of the design, implementation and analysis.
The analytical and statistical skills needed to tease out answers to policy questions from available data may exceed the capacities of a ministry of health. Some countries outsource the task of making sense of the quantities of health data to academic and research institutions.
For example, the Canadian Institute for Health Information (CIHI) is an independent, not-for-profit corporation whose vision is to be ‘a leading source of unbiased, credible and comparable information that will enable health leaders to make better-informed decisions.’ CIHI bases its reports on information provided by hospitals, regional health authorities, medical practitioners and government bodies.
The international community is collaborating to develop common frameworks and standards for data collection, analysis and dissemination for example, the Health Data Collaborative is a joint effort by multiple global health partners to work alongside countries to improve the availability, quality and use of data for local decision-making and tracking progress toward the health-related Sustainable Development Goals.
Contents
Source chapter
The complete chapter on which we based this page:

Macfarlane S.B., AbouZahr C., Tangcharoensathien V. (2019) National Systems for Generating and Managing Data for Health. In: Macfarlane S., AbouZahr C. (eds) The Palgrave Handbook of Global Health Data Methods for Policy and Practice. Palgrave Macmillan, London.
Additional resources
The United Nations Statistics Division repository of country profiles of statistical systems. This website contains a list of countries and organizations and includes a brief history of the country’s statistical system, legal basis, the statistical programme.
The Health Metrics Network (HMN) (2005-2013) supported countries to assess and develop plans to build strong health information systems. Its documents, including the HMN Framework and standards for country health information systems, can be found here: resources, country assessments and tools.
The Partnership in Statistics for Development in the 21st Century (PARIS21)promotes the better use and production of statistics throughout the developing world.
PARIS21. A Guide to Designing a National Strategy for the Development of Statistics (NSDS). This guide provides materials for the managers of national statistical systems develop and implement National Strategies for the Development of Statistics (NSDS).
MEASURE Evaluation has a mandate to strengthen health information systems in low-resource settings.
Routine Health Information Network (RHINO) was established to support strengthening of facility-based routine information systems particularly in low- and middle-income countries.
The Health Data Collaborative is a joint effort by multiple global health partners to work alongside countries to improve the availability, quality and use of data for local decision-making and tracking progress toward the health-related Sustainable Development Goals.
The 2015 Summit on Measurement and Accountability for Health issued a Call for Action which included a Roadmap to implement priority actions and targets to improve health measurement and accountability in LMICs.
Design and implementation of health information systems. A practical handbook describing the design and implementation of health information systems published by World Health Organization (written by Lippeveld and Sauerborn) in 2000.
United Nations. Handbook of statistical organization: The Operation and Organization of a Statistical Agency describes the operation and organization of a statistical agency.
United Nations Statistics Division publication of the Fundamental Principles of Official Statistics.
DHIS2 is an open source, web-based software platform for data collection, management, and analysis which is used by ministries of health in low- and middle-income countries.
Health facility and community data toolkit provides an overview of best practices, innovations, tools and methods that are available to countries in support of strengthening the components of a health facility information system.